

Is heroin ruining your life? Call: (855) 935-2871
HEROIN WITHDRAWAL SYMPTOMS
While it’s rare for heroin withdrawal to be actually life-threatening, the symptoms of withdrawal can make you feel terribly sick. These include:
- Nausea and stomach cramps
- Diarrhea
- Vomiting, sometimes to the point of dehydration
- Fever and chills
- Muscle spasms
- Pounding heart
- Agitation, depression or mood swings

Occasionally, someone experiencing withdrawal will experience convulsions, seizures or hallucinations.
HEROIN WITHDRAWAL TIMELINE
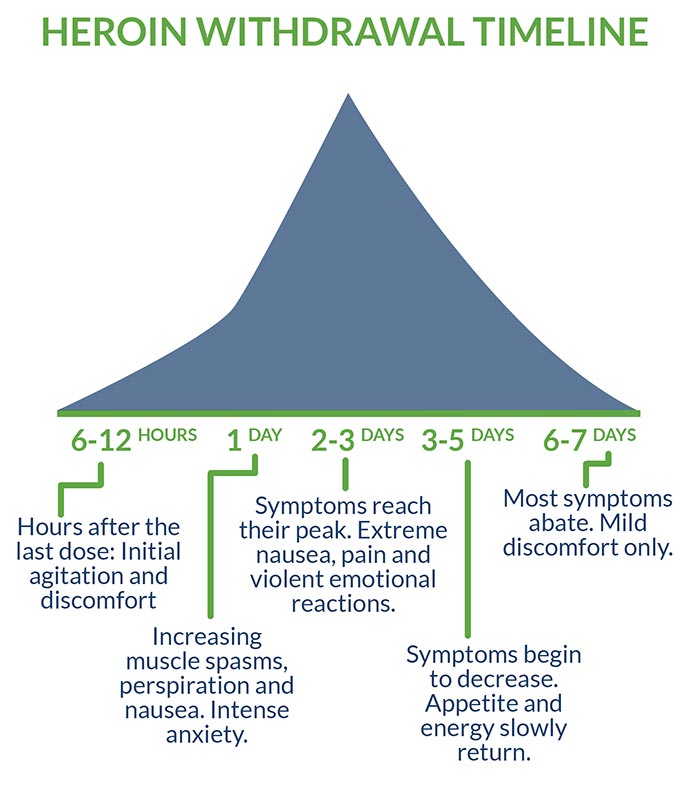
There are other differences in individual experiences of heroin withdrawal, but in most cases, physical withdrawal lasts about a week. Typically, the process goes like this:
- 6–12 hours after the last dose: Initial agitation and discomfort.
- 1 day: Increasing muscle spasms, perspiration, and nausea. Intense anxiety.
- 2–3 days: Symptoms reach their peak. Extreme nausea, pain, and violent emotional reactions.
- 3–5 days: Symptoms begin to decrease. Appetite and energy slowly return.
- 6–7 days: Most symptoms abate. Mild discomfort only.
Factors that affect intensity and duration of withdrawal include:
- The client’s overall physical condition
- The client’s mental and emotional condition
- How much heroin (or opiate drugs in general) has been taken, and for how long
INPATIENT TREATMENT FOR HEROIN
Even after physical detox, heroin cravings may recur periodically for several months. For this reason, ideally, three-plus months of follow-up care with daily therapy is recommended to prepare the patient for life without drugs. Getting support during this vulnerable period is an element in most recovery success stories.
Inpatient care, which involves residential hospitalization, is frequently recommended because:
- The client remains in a low-stress environment away from old temptations.
- Professional help is always close at hand.
- There’s no excuse for skipping therapy sessions due to fatigue or inconvenience.
- The client is in 24/7 close proximity to other people recovering from addiction, building everyday camaraderie and helping them feel less alone.
Inpatient care also allows ongoing supervision of anyone receiving Medication-Assisted Treatment to curb cravings. With heroin, there are special concerns here. Alternate opioid drugs, notably methadone, have been routinely used to reduce heroin-relapse cravings for decades, but—reminiscent of heroin’s earlier use in treating morphine addiction—also generate dependence issues of their own. Many former heroin addicts are now re-entering detox centers to get support and help to discontinue methadone, so it’s important that any program using alternate opiates includes a discontinuation plan.
Anyone without a solid support network on the outside almost certainly needs inpatient care. So does anyone living with the stress of a dual diagnosis (a mental illness in addition to the addiction).
OUTPATIENT TREATMENT FOR HEROIN
For all its advantages, inpatient care isn’t always practical for everyone. The pros of leaving residential treatment may outweigh the cons if someone:
- Has legitimate family, economic or vocational responsibilities on the outside and is prepared to cope with them. (It’s important to get input from a counselor before making this decision.)
- Is more comfortable in familiar surroundings, among familiar people. (This assumes the people are completely supportive and the surroundings free of potential relapse triggers.)
- Enjoys their work and finds its responsibilities an effective distraction.
A client whose situation matches that description still needs professional therapy and supervision for the first few months after detox. The solution may then be outpatient treatment, which involves regularly reporting to aftercare facilities. Most outpatient programs are based on one of the following models:
- Partial hospitalization: The client is onsite about six hours a day, five days a week.
- Intensive outpatient: The client is onsite three hours a day, three days a week.
- Transition: The client remains under inpatient treatment for the first month after detox, then moves to outside housing operated by the treatment center.
Most people in outpatient situations, especially if living beyond walking distance of the detox center, are more vulnerable to relapse than those in structured and supervised living environments. It’s important to have a detailed relapse-prevention plan, secure family support and arrange accountability for keeping all appointments.
CAN HEROIN DETOX BE DONE AT HOME?
Looking at everything involved in both inpatient and outpatient treatment, many people are tempted to think, “That sounds like an awful lot of trouble. Why can’t I just take a few sick days and quit cold at home?”
For one thing, just because heroin detox rarely kills outright doesn’t mean it’s safe. Some people become dehydrated from nausea and vomiting. Some become so frantic that they attempt suicide. The most likely danger, however, is that someone will yield to relapse cravings, put a fresh dose of heroin into a weakened body, and suffer a lethal overdose.
Even in the best-case scenario—a person has used opiates for a relatively short time, is in overall good health and has trustworthy support on hand—it’s virtually impossible to ensure the level of comfort, care, and safety available from medically supervised inpatient treatment. And even the home-detox success stories remain in significant danger of relapse without professional help to deal with the reasons behind the addiction, and without a support plan for dealing with a recurrence of cravings.
TAPERED VS. COLD TURKEY
Even in a clinical setting, there are varying opinions on the safest forms of detox. Many clinics opt for the cold turkey approach of cutting off all drugs and simply keeping the client comfortable, rather than risk possible complications from substitute opiates. However, hundreds of programs still opt for methadone to spare body and brain the full shock of heroin withdrawal: more than 356,000 opioid-addiction clients received methadone in 2015. The more preferable alternative to methadone: a short-term course of Suboxone, which increasingly is recognized as the gold standard of care when combined with behavioral therapies.
Treating heroin addiction with Suboxone is a form of tapering, which involves administering gradually reduced doses of a drug (or a safer substitute with similar effects) until a client is weaned from all cravings. Suboxone can be beneficial for patients at high risk for dangerous withdrawal symptoms or relapse. There is, however, real danger that people will treat these drugs simply as heroin substitutes and stay on them indefinitely, so it’s important to continue the tapering-off until a patient is opiate-free.
CONSIDERATIONS/HOW TO DECIDE WHAT IS RIGHT FOR YOU
Once a heroin detox client is clear on preferred medical approach, other factors to consider in choosing a treatment center include:
- Geographic location
- Philosophical and therapeutic approaches
- Facilities and programs for recovering clients
- Cost, including what health insurance will cover
Heroin rehab can cost hundreds of dollars a day, but even expensive centers are sound investments considering the costs of staying addicted: over $100 a day for the drug, plus damage to health, relationships, property and productivity.
RECOVERY SUCCESS AND AFTERCARE SERVICES FOR HEROIN
Unfortunately, dangers and potential costs don’t go away after addiction treatment. As with other chronic illnesses, around half of clients will have at least one subsequent relapse. Relapse doesn’t have to mean a return to full addiction, however: the true success stories are those who make ongoing progress and are happily sober in the long term.
Getting support, a vital part of heroin detox is also an important tool in avoiding relapse and in recovering from any relapses that do occur. Clients completing official heroin-addiction treatment are advised to continue with regular support in the forms of:
- An understanding with loved ones on what’s needed
- Long-term therapy for both client and family
- A primary care physician who understands the issues involved
- Peer support groups comprising other recovering addicts and their families
- Ongoing contact with the detox center
- Participation in continuing-care programs
- Membership in mental- and behavioral-illness organizations
Over 15,000 people in the United States now die each year from a heroin overdose. Addiction treatment saves lives.
For related information, see the following articles:
- “How Long Does It Take for Opiates to Leave Your System?”
- “Heroin Detox: What You Need to Know”
- “Preventing an Opiate Overdose with Naloxone”
- “Methadone Detox, Treatment and Addiction”
Is heroin ruining your life? Get help now
AddictionBlog.org. “The Cost of Heroin Addiction.” Retrieved from http://addictionblog.org/infographics/the-cost-of-heroin-addiction-infographic/
Gupta, Dr. Sanjay (2016, June 2). “Unintended Consequences: Why Painkiller Addicts Turn to Heroin.” CNN.com. Retrieved from https://www.cnn.com/2014/08/29/health/gupta-unintended-consequences/
Moghe, Sonia (2016, October 14). “Opioid History: From ‘Wonder Drug’ to Abuse Epidemic.” CNN.com. Retrieved from https://www.cnn.com/2016/05/12/health/opioid-addiction-history/index.html
National Institute on Drug Abuse (2017, September). “Overdose Death Rates.” Retrieved from https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
National Institute on Drug Abuse (2018, January). “How Effective Is Drug Addiction Treatment?” Retrieved from https://www.drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/frequently-asked-questions/how-effective-drug-addiction-treatment
National Institute on Drug Abuse (2018, June). “What Is the Scope of Heroin Use in the United States?” Retrieved from https://www.drugabuse.gov/publications/research-reports/heroin/scope-heroin-use-in-united-states
Substance Abuse and Mental Health Services Administration (2017, August 22). “SAMHSA Report Shows Increase in Opioid Treatment Facilities.” Retrieved from https://www.samhsa.gov/newsroom/press-announcements/201708220100
United Nations Office on Drugs and Crime (1953, January 1). “History of Heroin.” Retrieved from http://www.unodc.org/unodc/en/data-and-analysis/bulletin/bulletin_1953-01-01_2_page004.html
United States Drug Enforcement Administration. “Drug Scheduling: Drug Schedules.” Retrieved from https://www.dea.gov/druginfo/ds.shtml
U.S. Food and Drug Administration (2018, May 16). “FDA Approves the First Non-Opioid Treatment for Management of Opioid Withdrawal Symptoms in Adults.” Retrieved from https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm607884.htm




