

TABLE OF CONTENTS
- Introduction to Methadone Detox
- Methadone Withdrawal Symptoms
- Methadone Withdrawal Timeline
- Inpatient Treatment for Methadone
- Outpatient Treatment for Methadone
- Can Methadone Detox Be Done at Home?
- Tapered vs. Cold Turkey
- Considerations for Methadone Detox
- Recovery Success and Aftercare Services for Methadone
 Methadone’s widespread use as a transition drug to help wean users off other opiates, most notably heroin, has created a deadly epidemic prompting calls for greater regulation of the drug:
Methadone’s widespread use as a transition drug to help wean users off other opiates, most notably heroin, has created a deadly epidemic prompting calls for greater regulation of the drug:
- According to the Centers for Disease Control and Prevention (CDC), methadone overdoses kill approximately five thousand people annually— and, although methadone represents only 2 percent of opiate painkillers prescribed in the US, the drug has been implicated in a third of those overdose deaths.
- Many experts report that methadone is the most addictive, unpredictable and deadly of all opiates.
- Mounting concerns about its dangers prompted the Food and Drug Administration (FDA) to require a “black box” warning on all labels, starting in 2006. In 2008, the Drug Enforcement Administration (DEA) pressured manufacturers to limit sales to hospitals and addiction clinics as part of a new initiative.
Is methadone ruining your life? Call: (855) 935-2871
METHADONE WITHDRAWAL SYMPTOMS
Methadone targets the same brain receptors as other opiates. Through a binding process, the drug works to dull the perception of pain, inducing short-term euphoria and setting the stage for addiction. Long-term methadone dependence is dangerous because of the unpredictable interactions and tolerance the drug creates in users—many of whom use other opiates. Even casual recreational use may result in dependency and significant withdrawal symptoms.
Methadone withdrawal requires professional medical evaluation and management. Clients are administered various physical and psychiatric assessments prior to beginning treatment, and specialized tools like the Clinical Opiate Withdrawal Scale (COWS) help determine the severity of symptoms based on scores. The scores obtained during the evaluation then inform medication-assisted treatment (MAT) and determine client-specific therapy. Depending upon the frequency, duration and intensity of use, clients may experience the following cluster of early and late stage withdrawal symptoms:
- Disorientation
- Lightheadedness
- Nausea
- Restlessness
- Insomnia
- Chills
- Mood swings
- Irritability
- Dilated pupils
- Muscle and joint pain
- Exhaustion
- Diarrhea
- Vomiting
- Fatigue
Methadone WITHDRAWAL TIMELINE
Methadone’s long-acting properties accumulate quickly in the majority of users and present a unique danger. Unlike other opiates, even taking one additional dose of the drug can result in an overdose or complicate the withdrawal process. This is, in part, explained by methadone’s depressant effect on the heart and lungs—which continues long after its pain-relieving effects have subsided. Methadone has an unusually long and variable half-life of approximately 8-60 hours.
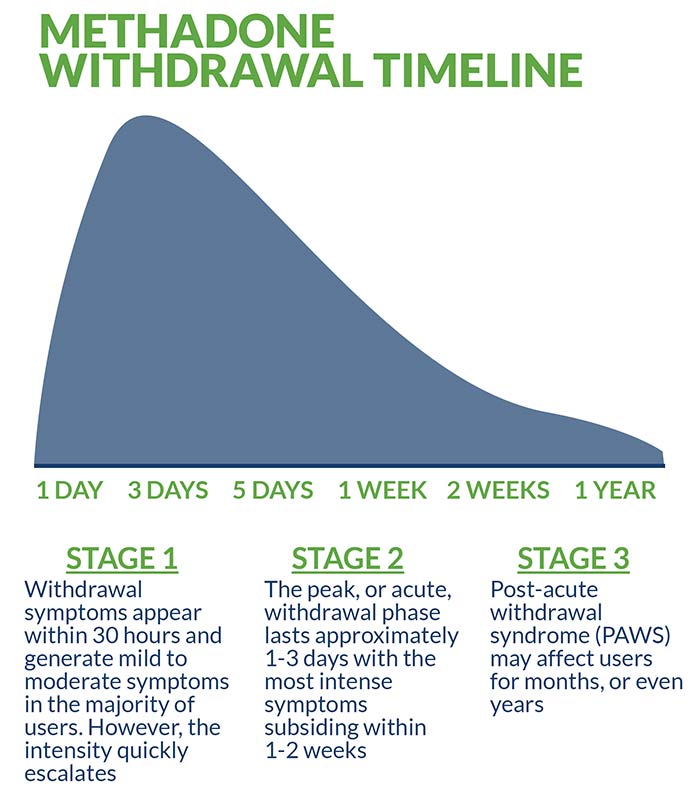
Typically, withdrawal symptoms appear within 30 hours following dosage and generate mild to moderate symptoms in the majority of users. However, the intensity quickly escalates. The peak, or acute, withdrawal phase lasts approximately one to three days with the most intense symptoms subsiding within one to two weeks. The third, and final, stage of methadone withdrawal is known as post-acute withdrawal syndrome (PAWS) and its diminishing effects may impact users for months, or even years. In rare cases, permanent damage is sustained as a result of the drug’s potency and unpredictable interactions with other opiates.
Methadone is detectable in blood tests for approximately 24 hours, whereas urine tests register traces for up to 12 days. Hair follicle testing provides the longest range of detection, in some cases appearing for over three months following dosage.
INPATIENT TREATMENT FOR METHADONE
Intensive inpatient treatment is the industry-preferred standard for methadone detox. This popular treatment option involves clients living at a designated facility for the duration of treatment during which time they receive licensed medical supervision, ongoing medication management and regular psychotherapy. Many inpatient treatment facilities feature an impressive list of benefits and services, including 24/7 staff monitoring and comprehensive aftercare planning.
Medication-Assisted Treatment
Medication-assisted treatment (MAT) describes the use of Food and Drug Administration (FDA) approved pharmacological interventions in combination with psychotherapy. Evidence- based therapies frequently include cognitive behavioral therapy (CBT), dialectical behavioral therapy (DBT), motivational interviewing (MI) and trauma-informed therapy. In cases where presenting problems involve the family unity, ongoing family therapy may be recommended and incorporated into the treatment protocol.
Administering methadone in tapering doses during detox is a controversial practice. Due to the highly addictive properties of the drug, proper caution must be taken before resorting to this method. Generally, supplemental medication is used as a foundation to guide safe treatment. According to the National Alliance of Advocates for Buprenorphine Treatment (NAABT) carefully controlled doses of the following evidence-based medications are considered optimal:
- Suboxone provides a controlled, long-lasting dose of opiates without producing the same euphoric high as methadone.
- Subutex produces a similar but less potent effect when compared to methadone which helps in reducing withdrawal symptoms and diminishing cravings.
Dual-Diagnosis Treatment
Anxiety and depression-related disorders are often precursors to methadone addiction and polysubstance abuse. Post-traumatic stress disorder is also a known precipitating factor that leads many users to self-medicate. These co-existing, or “co-occurring” disorders as they are often called, require professional medical management and psychotherapy to effectively address. Depending upon a client’s specific diagnoses and presenting issues, medications including pregabalin, buspirone, gabapentin and SSRIs are incorporated into the treatment regimen in addition to the aforementioned primary detox medications.
OUTPATIENT TREATMENT FOR METHADONE
Outpatient treatment is an affordable alternative to inpatient treatment that involves transitional care. In outpatient settings, found in various public and private institutions, clients receive less intensive care and do not live at the facility 24/7. Particularly attractive to clients with demanding personal and professional schedules, outpatient treatment offers many of the same services and benefits as inpatient treatment on a less comprehensive basis.
CAN METHADONE DETOX BE DONE AT HOME?
Methadone is a potent, unpredictable opiate that should never be treated at home. Self-guided detox is statistically proven to lead to unfavorable treatment outcomes, a greater likelihood of future relapse and exposes users to potentially deadly risks. Even casual recreational users benefit from the help of an established treatment protocol and, in more severe cases, medical supervision and medication management are a necessity.
TAPERED VS COLD TURKEY
Quitting methadone cold turkey is extremely dangerous and should never be attempted under ANY circumstances. Doing so increases the likelihood of “precipitated withdrawal,” the rapid intensification and acceleration of withdrawal symptoms. As noted above, methadone “dose tapering” is a highly controversial treatment method that subjects the body to the very same substance that created and sustained the addiction. For this reason, carefully controlled doses of other evidence-based medications like Suboxone and Subutex—and only as a short-term treatment intervention—is deemed the safest and most effective approach.
CONSIDERATIONS/HOW TO DECIDE WHAT IS RIGHT FOR YOU
The decision to enter methadone detox and rehabilitation is critical, and individual variables such as location, affordability, insurance coverage, spirituality, and facility reputation must all be considered. The majority of facilities will be able to verify insurance coverage and benefits prior to enrollment which helps ensure a stress-free admission process. In most cases, full or partial coverage is granted. In the unusual event that coverage is denied, additional financial options will be discussed. These include federal grants, private scholarships and other forms of need-based aid.
RECOVERY SUCCESS AND AFTERCARE SERVICES FOR METHADONE
Empirical evidence suggests that successful completion of inpatient detox is only one necessary component of long-term sobriety. Other factors dictating long-term success rates fluctuate depending upon individual client motivation and strict adherence to a relapse prevention strategy that involves:
- Narcotics Anonymous and 12-step involvement
- Continuing medication management
- Healthy diet
- Regular physical activity
- Sponsorship
- Life and job skills coaching
- Random drug testing
- Regular sober peer support
- Abstinence from triggers
Also, remember that methadone overdose is considered a life threatening medical emergency. In the event of overdose— immediately seek professional medical help at a hospital emergency room (ER).
Is methadone ruining your life? Get help now
Related Articles :
How Long Does Methadone Withdrawal Last




