

Understanding Suboxone
What Is Suboxone?
Suboxone is a brand name medication that combines buprenorphine and naloxone to treat opioid use disorder.
- Buprenorphine
A partial opioid antagonist that helps reduce withdrawal symptoms and cravings without causing a full “high.” - Naloxone
An opioid antagonist that blocks the pleasurable effects of opioids (e.g., pain relief and euphoria) and deters misuse.
Why Suboxone Is Used in Addiction Treatment
Suboxone reduces opioid cravings, minimizes withdrawal symptoms, and lowers the risk of relapse satisfying the brain’s need for opioids in a controlled, less euphoric way.
While Suboxone can be life-changing for many, stopping it too quickly (or without proper medical supervision) can lead to uncomfortable withdrawal symptoms.
What Are the Symptoms of Suboxone Withdrawal?
Common Symptoms of Suboxone Withdrawal
Suboxone withdrawal symptoms may resemble heroin withdrawal, though they are generally milder:
- Anxiety
- Body aches
- Cramping
- Diarrhea
- Dilated pupils
- Gooseflesh skin
- Headaches
- Increased heart rate
- Insomnia
- Intense opioid cravings
- Irritability
- Mood swings
- Nausea
- Sweating
- Vomiting
- Yawning
Psychological and Physical Effects of Suboxone Withdrawal
Suboxone withdrawal symptoms impact the body and mind, which often interfere with daily responsibilities and increase the risk of relapse if they’re not properly managed.
Physical symptoms may include:
- Flu-like symptoms
- Body aches
- Chills
- Upset stomach
Psychological symptoms may include:
- Anxiety
- Irritability
- Intense cravings
Early Signs of Suboxone Withdrawal
- Anxiety
- Irritability
- Runny nose and tearing
- Sweating
- Trouble sleeping
- Muscle aches
These symptoms often increase in severity for the first 72 hours as the withdrawal progresses.
Severe Symptoms of Suboxone Withdrawal
In more severe cases, withdrawal symptoms may include:
- Intense drug cravings
- Nausea and vomiting
- Diarrhea and dehydration
- Depression or suicidal thoughts
- Inability to function at work, school, or home
Suboxone Withdrawal Timeline
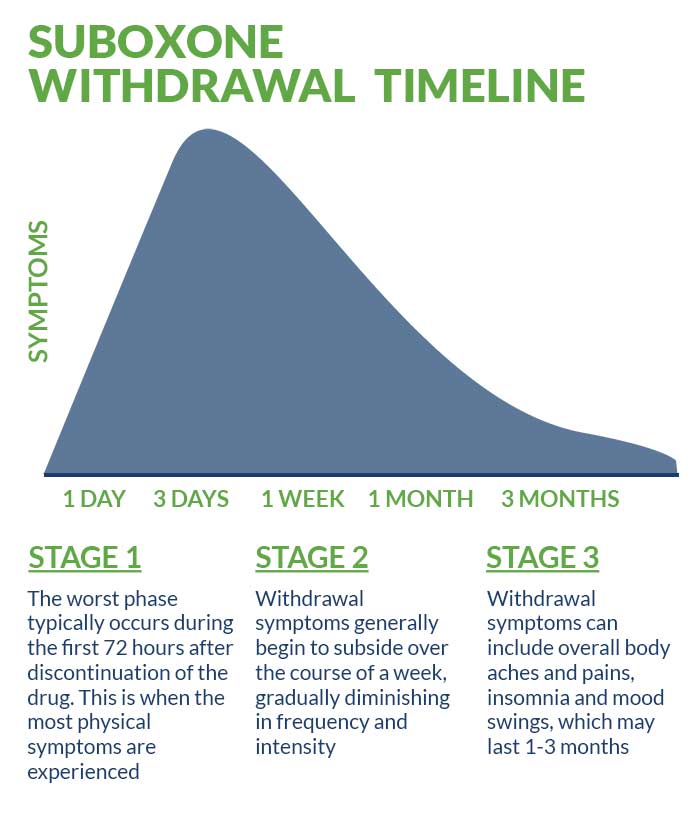
How Long Does Suboxone Withdrawal Last?
Suboxone’s long half-life (ranging from 36 to 72 hours) means withdrawal typically begins one to three days after the last use, with peak symptoms around day three.
Drug test detection windows:
- Urine
Buprenorphine is detectable in urine within 40 minutes of taking the drug and can remain detectable for up to two weeks. (Most buprenorphine is excreted via feces, while 10-30 percent is excreted in urine.) - Blood
Suboxone stays in the blood for 2-10 hours after the last dose. A blood test can detect same-day usage of Suboxone. - Saliva
Saliva tests of Suboxone users can detect the presence from 3-10 days after use. - Hair
Metabolites of Suboxone (principally norbuprenorphine) can be found in hair for up to three months after last use.
While acute withdrawal symptoms usually resolve within a week, lingering symptoms like mood swings, sleep issues, and low energy may last for one to three months.
Other Factors That Influence Withdrawal Duration
- Age
- Weight
- Body fat percentage
- Overall physical health
- Length and dosage of Suboxone use
- Co-occurring mental health conditions
Long-term Suboxone users have a higher risk of depression or an anxiety disorder (that may or may not have been precipitated by withdrawal symptoms) that persists for months.
How to Get Off Suboxone Safely
Gradual Tapering vs. Abrupt Discontinuation
Stopping “cold turkey” can be dangerous and potentially fatal depending on how long and how much you’ve been using. A gradual taper that’s guided by a medical professional is safer and more effective.
Consulting a Healthcare Professional for Safe Detox
Working with a Beach House Center for Recovery addiction specialist ensures you’ll receive a personalized and medically supported Suboxone detox guide.
What Helps With Suboxone Withdrawal: Best Practices
- Stay hydrated
- Eat balanced, nutrient-rich meals
- Get 7-9 hours of restorative sleep each night
- Seek emotional support from counselors and loved ones
Suboxone Withdrawal Treatment Options
Medications to Ease Suboxone Withdrawal
Several Suboxone withdrawal medications can help ease symptoms during detox, including:
- Anti-nausea medications
- Sleep aids
- Non-opioid pain relievers
Behavioral Therapy and Counseling for Suboxone Detox
At Beach House Center for Recovery, we understand that addiction and mental health are often entwined. That’s why we provide the following therapeutic offerings in our treatment programs:
- Cognitive Behavioral Therapy (CBT)
- Dialectical Behavioral Therapy (DBT)
- Motivational Interviewing (MI)
- Integrated Trauma Treatment
What Is Suboxone Detox Medication and How It Helps
Suboxone detox medications such as clonidine or lofexidine may help:
- Suppress acute withdrawal symptoms
- Reduce anxiety and physical discomfort
- Ease mood swings
How to Deal With Suboxone Withdrawal
Self-Care Strategies During Withdrawal
You can support your medically assisted detox program and help ease discomfort by engaging in these self-care strategies:
- Participating in regular physical activity
- Keeping a structured routine
- Engaging in mindfulness practices (e.g., yoga, meditation, journaling, etc.)
Seeking Professional Help: When to Get Assistance
If you or your loved one have tried detoxing from Suboxone or other opioids alone without success, are experiencing severe symptoms, or have intense cravings that are putting you at risk for relapse, seeking professional help is critical for your safety and long-term recovery.
Suboxone Detox Programs: What You Need to Know
Inpatient vs. Outpatient Detox Programs
Everyone’s detox needs are unique and require a tailored approach. We can help you determine whether an inpatient or outpatient detox program is right for you. All of our detox clients receive high-quality, personalized treatment and daily check ins with our addiction specialists.
- Inpatient clients receive 24/7 monitoring and care
- Outpatient clients check in daily but return home at night
Can Suboxone Detox Be Done at Home?
We strongly advise against attempting to detox at home. The risk of relapse, overdose, or unmanaged withdrawal is high, especially without knowing how to safely taper.
A medically supervised detox program ensures you’re monitored, supported, and protected every step of the way.
Don’t take the risk. Call Beach House Center for Recovery today and take the first step toward safe, compassionate, and professional Suboxone detox and recovery.
Benefits of a Suboxone Detox Program for Withdrawal Management
A medically supervised detox program for Suboxone offers:
- Around the clock clinical support for physical and mental symptoms
- Medication management
- A secure, drug-dree environment to reduce relapse risk
- Access to counselors and peer support
- Seamless transition to long-term Suboxone addiction treatment and recovery care
What to Expect During Suboxone Detox
When undergoing medical detox at Beach House Center for Recovery, you can expect:
- Regular health assessments
- Medications to reduce symptoms
- Regular monitor and medication adjustments to optimize healing
- Nutritional support and hydration
- Emotional support from counselors and recovery specialists
- A calm, supportive, and non-judgmental environment
Tapered vs. Cold Turkey: Which Detox Method Is Right for You?
The Dangers of Abruptly Stopping Suboxone (Cold Turkey)
Quitting Suboxone suddenly can shock the system, triggering intense withdrawal symptoms and relapse.
Why Gradual Tapering is the Safer Option
Gradual tapering allows your body to slowly adjust to lower doses of Suboxone over time. When done under medical supervision, this method can:
- Minimizes withdrawal symptoms
- Reduces relapse risk
- Offers physical and emotional support
Working closely with your Beach House Center for Recovery addiction specialist ensures the tapering plan is tailored to your needs, ensuring the Suboxone withdrawal process is manageable and safe.
Considerations for Choosing the Right Detox Method
How to Decide Between Inpatient and Outpatient Treatment
Choosing between inpatient and outpatient detox is a personal decision. It should be based on your
- Home environment
- Medical and mental history
- Previous detox attempts
- Financial situation
While finances shouldn’t be the only factor, we understand cost is a major concern for many. Financial help may be available through federal, state and local programs. Some treatment facilities also offer sliding scale fees, payment plans, or financing options to reduce out-of-pocket expenses.
The most important question to ask yourself is: “Where will I receive the safest, most supportive care for my recovery?”
Factors to Consider for a Safe Detox Journey
- Do you have a stable and supportive home environment for outpatient care?
- Have you tried quitting before without success?
- Are you managing co-occurring mental health conditions?
- Would a structured, 24-hour environment (e.g., inpatient care) help you stay on track?
- Are there resources available to help cover costs, such as the Veterans Administration (VA) or public health programs?
Taking time to consider your needs and explore your options can help ensure you select the best path for your needs.
Recovery Success and Aftercare Services for Suboxone Detox
How Aftercare Programs Aid in Long-Term Recovery
Aftercare is an essential part of recovery and supports long-term sobriety after medical detox.
Our continuing care program helps you:
- Identify and manage triggers
- Build effective coping skills for long-term recovery
- Maintain accountability
- Receive ongoing support for mental health conditions
Steps to Maintain Sobriety After Suboxone Detox
Here’s how you can maintain sobriety after Suboxone detox at Beach House Center for Recovery:
- Stay involved in our continuing care program and therapy
- Find and engage with a supportive sober community
- Maintain a healthy and structured daily routine
- Use coping strategies to manage stress or cravings
Is Suboxone ruining your life? Get help now
Related Articles:
How Long is Suboxone Withdrawal?
How Long Does Suboxone Withdrawal Last?